Clinical benefits and economic cost-savings of remote electrical neuromodulation (REN) for migraine prevention
Robert Cowan et al, Journal of Medical Economics, 2022
ABSTRACT
Aims: Assess the clinical benefits and associated direct and indirect cost-savings from Remote Electrical Neuromodulation (REN) for migraine prevention.
Methods: REN, a prescribed, wearable, FDA-cleared neuromodulation-device for acute and/or prevent- ive treatment of migraine, recently demonstrated efficacy for migraine prevention when used every- other-day, in a prospective, randomized, double-blind, placebo-controlled, multi-center study. Following baseline (4-weeks), subjects underwent treatment with REN or placebo (8-weeks), and elec- tronically reported migraine symptoms and acute treatments daily. Therapeutic-gain was the between- groups difference (REN minus placebo) in change from baseline to the second month of intervention. Health-economics impact was derived as cost-savings associated with REN’s clinical benefits.
Results: Out of 248 subjects randomized (128 active, 120 placebo), 179 (95:84) qualified for modified intention-to-treat (mITT) analysis. Significant therapeutic gains favoring REN vs. placebo were found (Tepper et al. 2023), including mean (±SD) reduction in number of acute medication days (3.5±0.4 vs. 1.2±0.5; gain = 2.2; p = .001) and presenteeism days (2.7±0.3 vs. 1.1±0.4; gain = 1.6, p= .001). Mean changes of provider visits (reduction of 0.09±0.1 vs. increase of 0.08±0.2; p= .297), and reduction of absenteeism days (0.07±0.1 vs. 0.07±0.2; p = .997) were not significant. Mean annual cost-saving for one patient using REN for migraine prevention estimated $10,000 (±$1,777) from reductions in these four clinical outcomes relative to baseline without REN treatment. Extrapolated to a hypothetical US commercial health-plan of one-million covered lives, assuming the national prevalence of migraine patients on preventive treatment, annual mean (±SE) cost-saving from using REN migraine prevention estimated $560.0 million (±$99.5 million) from reduction in direct (~$330 millionm) and indirect costs (~$230 millionm) measured.
Limitations: Clinical and cost-savings benefits presented are conservative, assessed only from end- points measured in the clinical trial. Moreover, some of the endpoints had only scarce or no occur- rences during the study period.
Conclusions: Coverage of the REN-device for migraine prevention may significantly reduce disease- burden and save a one-million-member payer plan at least $560 million per year.
PLAIN LANGUAGE SUMMARY
Migraine affects more than 1 billion people worldwide, causing significant disability and substantial clinical economic burden. Remote Electrical Neuromodulation (REN) is a prescribed, wearable, non-pharmacological, non-invasive device (Nerivio), indicated for acute and/or preventive treatment of migraine with or without aura in patients 12 years and older. Efficacy of REN for migraine prevention was recently demonstrated in a randomized, blinded, placebo-controlled clinical-trial. This study further analyzes clinical benefits from end- points measured in the clinical-trial as well as their associated direct and indirect costs. Out of 248 subjects randomized (128 active, 120 placebo), 179 (95:84) qualified for modified intention-to-treat (mITT) analysis. Significant therapeutic gains favoring REN over placebo were found, including an average reduction of 3.4 acute medication days/month, and an average reduction of 2.7 presenteeism days/month. A reduction in the number of provider visits and absenteeism days was also reported, though not significantly differed from changes in the control group. Mean annual cost-saving from reductions in these four clinical outcomes relative to baseline without REN treatment for a patient using REN for migraine prevention estimated $10,000. Extrapolated to a hypothetical US commercial health-plan of one million covered lives, annual mean cost-saving from using REN for migraine prevention is estimated to be $560.0 million, composed of $327.8 million direct costs and $232.2 million indirect costs. Thus, REN preventive treatment for migraine reduces disease burden and leads to meaningful cost-saving, both direct and indirect, proposing clinical and financial incentives for patients, health insurance systems, and employers to utilize REN for migraine prevention.
Introduction
Migraine is a highly debilitating condition with a global prevalence of 14% causing substantial economic burden on the healthcare system and on employers in the United States. According to an analysis of US healthcare claims filed during 2007–2013, the annual direct healthcare costs for individuals with migraine were estimated at $22,364 per person, compared to $15,697 for individuals without migraine (adjusted for inflation with 2019US$). Migraine is also associated with substantial indirect cost due to lost pro- ductive-time, including absenteeism (days of missed work) and presenteeism (days worked with diminished productivity due to functional disability). Moreover, migraine can lead to medication overuse, poor quality of life, chronic disabil- ity, and more. The indirect annual cost associated with migraine in the US has been estimated at $19.3 billion. This excludes presenteeism, which adds large indirect costs, espe- cially to employers. Given the high prevalence and disabling nature of migraine, it is particularly important for employers to be aware of the severity of economic burden that migraine puts on their workforces, and to inform payors and insurers the importance of impactful migraine management in reducing this burden.
Migraine treatments include acute treatments – applied upon the onset of an attack to abort symptoms, and pre- ventive therapies – intended to reduce the number of migraine and headache days. Use of preventive migraine treatment has been shown to decrease the utilization of healthcare resources, resulting in lower overall healthcare costs, as well as reduced migraine-related productivity losses. Despite this evidence, preventive migraine treat- ments are underutilized. According to a 2021 consensus statement by the American Headache Society (AHS), only 3– 13% of individuals with migraine use preventive treatment, even though nearly 40% of those with migraine, and almost all chronic migraine patients, would potentially benefit from it. The AHS 2021 consensus further notes that the poor adherence to treatment is caused by the fact that many oral preventive treatments have low-to-moderate efficacy, moder- ate-to-high rates of adverse events, contraindications, and/or pharmacological interactions. Low adherence could also result from limited access to non-generic preventive drugs which require failure on generic drugs in addition to being costly.
Remote electrical neuromodulation (REN) is a migraine treatment which stimulates upper arm peripheral nerves to induce conditioned pain modulation (CPM) – an endogenous analgesic mechanism that is deficient in people who suffer from migraine, fibromyalgia, and certain other neurological diseases. The efficacy of REN as an acute treatment for migraine was previously established in adults with chronic and episodic migraine, and in adolescents. These findings were further supported by a real-world ana- lysis of over 23,000 treatments, indicating that REN pro- vides a safe and efficacious abortive migraine treatment. Additional support for REN’s efficacy in acute treatment of migraine comes from meta-analysis studies, with the Agency for Healthcare Research and Quality Methods (AHRQ) report- ing REN has moderate strength of evidence (SOE), and that REN is the only neurostimulation device with enough evi- dence-based research supporting its efficacy for acute treat- ment for migraine. Moreover, the American Headache Society (AHS) consensus statements recommends REN as one of the second-line acute treatments for those who do not respond to the first-line triptan or for whom the first-line treatment is intolerable or contraindicated.
Recently, a large randomized, double-blind, placebo-con- trolled study further examined the clinical efficacy and safety of REN for preventive treatment of migraine. REN was sig- nificantly superior to placebo device (sham stimulation) in the primary endpoint – reduction in mean (±SD) number of migraine days per month (4.0±4.0days in the REN group vs.1.3±4.0days in the placebo group, therapeutic gain = 2.7days, p < .001), and in all prospective secondary end- points – reduction in mean number of moderate/severe headache days, reduction in mean number of headache days, percentage of patients whose headache days were reduced by at least 50%. Blinding analysis showed high level of participant blinding to their randomized therapy.
This health economics and outcomes research (HEOR) study further analyzed aspects of the above-mentioned trial, focusing on the financial impact associated with REN preventative treatment. Direct healthcare costs related to migraine treatment measured in the study include reduction in acute medication days, and migraine related medical care (healthcare provider appointments, emergency room visits, brain scans, inpatient admission). Indirect costs include lost productive-time due to migraine causing absenteeism days (number of missed work/school days), and presenteeism days (number of work/school days with moderate/severe functional disability). Direct and indirect estimates are summed up to assess the total annual economic burden of REN migraine prevention for the employer, per patient, and for a hypothetical US commercial health plan of one million covered lives.
Methods
Participants
The clinical trial (Clinicaltrials.gov NCT04828707; see) was conducted at 15US centers. Eligible patients were 18– 75years old with at least 6months of diagnosed migraine meeting the International Classification of Headache Disorders, 3rd edition (ICHD-3) diagnostic criteria for migraine with or without aura, with either chronic or epi- sodic migraine; 6-24 headache days and at least 4 migraine attacks per 28-days month, aka 4weeks. Before and through-out the study, subjects either did not use preventive medica- tions or were on a stable dose of a single migraine preventive medication. The study was approved by Western Institutional Review Board (WIRB; 20210751) and was con- ducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their enrollment (For further details see).
Study design
The clinical trial was a prospective, randomized, double- blind, placebo-controlled, multi-center trial. The ratio between active and placebo groups was 1:1, stratified at 1:1 ratio between episodic migraine patients (6–14 headache days per four weeks) and chronic migraine patients (15–24 headache days per four weeks), based on reports from the baseline phase. All participants were naïve to REN.
Participants reported daily in a migraine/headache diary in the smartphone app connected to the REN device (NerivioVR; Supplementary Appendix 1). Collected data included head- ache severity using a 4-point scale (none, mild, moderate, severe); presence/absence of aura and associated migraine symptoms; functional disability using a 4-point scale (no limi- tation, some limitation, moderate limitation, severe limitation); acute migraine medication intake (whether taken, and if so, the type of medication); migraine related medical-care (neur- ologist appointment, other healthcare provider appointment, emergency room visit, brain imaging procedure, inpatient admission); and days of missed school/work (absenteeism).
The study consisted of two phases:
1. Baseline (4-weeks; weeks 1-4): participants used their usual migraine medications when needed and com- pleted a daily diary report.
2. Intervention (8-weeks; weeks 5-12): Eligible patients were randomized in a 1:1 ratio to active:placebo blinded groups. Participants were instructed to continue daily diary recording, to conduct a full 45-minute treatment with their assigned device (REN or placebo) every-other- day, and to treat their migraine/headaches with their usual acute medications. Eligibility to participate in this phase required: 6–24 headache days during the baseline period; at least 4 migraine days during baseline; and completion of the diary on at least 22 out of the four baseline weeks (80% compliance).
Study device
The active REN (Nerivio) device produces a proprietary pulse with a modulated frequency of 100–120Hz, and up to 40mA output current. The placebo device produces electrical pulses of the same maximum intensity, but with lower frequency and pulse duration.Participants were instructed to modulate the intensity level (device output current) during each treatment (active/placebo) so that the stimulation felt strong yet not painful. Treatment duration was 45min.
Clinical outcome measures
The current analysis focuses on the financial impact of the intervention (for primary and secondary clinical outcomes, see). All endpoints are presented per-month (calculated over 4-weeks, similarly to other migraine prevention studies). Given that preventive processes may require time to exert their effect, only data from the last 4weeks of the intervention phase (weeks 9–12) were included in the statistical analysis(common timeframe for efficacy analysis in migraine prevention studies, e.g. Rimegepant, Erenumab, Vagus nerve stimula- tion) and compared to the baseline phase (weeks 1–4).
The following endpoints were examined, testing the mean change from baseline to the second month of inter- vention in the number of:
1. acute headache/migraine medication days;
2. headache/migraine related healthcare provider (HCP) appointments (sum of neurologist/pain-specialist appointments and other HCP appointments);
3. headache/migraine related ER visits;
4. headache/migraine related brain scans;
5. headache/migraine inpatient admissions;
6. absenteeism days (number of missed work/school days);
7. presenteeism days (number of days with moderate/se- vere functional disability without absenteeism). Difference between the groups (i.e. the therapeutic gain, REN minus placebo) were calculated.
Health economics analyses
In clinical practice, from the patients’ perspective as well as for payors, the relevant clinical and financial metrics are changes resulting from the use of a therapy as opposed to not using that therapy. Therefore, the mean cost-savings per clinical outcome was calculated for the REN group by first evaluating the difference between baseline (reflecting the absence of REN treatment) to the second month of active treatment for each endpoint. The difference was then multi- plied by its corresponding average cost (see below the sour- ces of estimated averages costs). Results were extrapolated for a hypothetical US commercial health plan of one million covered lives over one year to provide meaningful econom- ics metrics. One million members is a common US payer size and is often used in health economics evaluations because it is easily scalable to an individual payer’s plan. The estimated prevalence of migraine of 14.0% was taken from a recent, large scale, review study of 357 publications. The portion of migraine patients who could benefit from preven- tion treatment, namely 40% of migraine patients, was taken from the latest American Headache Society consensus state- ment. Thus, for a hypothetical payor with 1 million covered lives, there are 56,000 migraine patients eligible for prevent- ive treatment. The formula used for annual health economics analyses was, per every endpoint, as follows:
mean cost - savings = change from baseline to 2nd intervention month × average unit cost × 1; 000; 000 lives covered × 0.14 portion of covered - lives with migraine × 0.4 migraine patients who should be on migraine preventives × 12 months = change from baseline to 2nd intervention month × average unit cost × 56; 000 covered patients eligible for migraine prevention
Average costs (per endpoint per unit) were estimated based on the following:
Acute medication day cost ($120.2)
Weighted average of acute treatments for migraine (costs taken from Price Intelligence (POLI) by GlobalData Plc, December 2021), accounting for the actual market share (portion of sales) per acute medication type (migraine sales data from IQVIA for Q4 2021).
Absenteeism day ($224.0)
US Bureau of Labor Statistics, national employment and wage data over all occupations, May 2021, assuming eight work hours per day (hourly wage of $28.0).
Presenteeism day ($112.0)
In the absence of precise information on the magnitude of productivity loss per each day of presenteeism, we adopted the measure used by Shimizu et al. 2021, assuming work efficiency is halved on presenteeism days. The mean cost per unit was therefore half of that calculated for absentee- ism days.
Provider appointments ($323.0)
We considered the main providers who typically treat people with migraine: primary care/family physicians at first, and then neurologists, with a 50:50 split. National mean expense for an office-based HCP visit, adjusted for inflation to 2022US dollars from 2016 according to the Medical Expenditure Panel Survey (MEPS) 2016 data, is $218 for primary care/family physicians and $428 for neurologists (represented in the “other” category in the MEPS database). Thus, the average cost of physician appointment for migraine patients used in the analysis is $323.
Analysis sets
The intended-to-treat (ITT) dataset included all randomized subjects and served as the dataset for safety assessments. The pre-defined analysis set consisted of the modified intended-to-treat (mITT) group. Specifically, these were par- ticipants with at least 22 daily reports and at least 12 treat- ments performed in the last four weeks of the intervention phase.
Sub-analysis
We further conducted a separate sub-analysis for subjects using one migraine-prophylaxis therapy (in addition to REN) vs. those not using any migraine-prophylaxis.
Statistical analysis
Between-groups differences were compared with independ- ent t-tests (continuous variables) and chi-squared tests (nominal variables). All tests were two-tailed. Data were ana- lyzed using IBM-SPSS statistics software version 28.0.
Data from participants with less than 28 report days/per- iod was standardized to 28days, for all efficacy endpoints.
Results
Participants demographics
The study was conducted between 13 April 2021, and 11 August 2022. Out of 335 enrolled subjects, 248 subjects (74%) were eligible at the end of the baseline phase. These subjects were randomized and received a device (128 active: 120 placebo). Of these, 179 (72.2%) were included in the mITT (95 active: 84 placebo). Participants were 86% female, had a mean age of 41.7 (SD = 12.9), 25.0% had migraine with aura, the ratio between episodic and chronic migraine was 48.4:51.6%, and 40.8% used a preventive medication in addition to REN. Half of the preventive medication users were on first-line preventives (i.e. generic oral drugs), and the other half were on second-line preventives (i.e. anti-CGRP mAbs, onabotulinumtoxinA, and gepants) meaning they had failed first-line preventives in the past. The REN and placebo arms did not differ in the distribution of types of preventives medications (p=0.413 in mITT, 0.240 in ITT). Full demo- graphic and clinical characteristics of the study participants are presented elsewhere.
Clinical outcomes
Mean change from baseline to the second month of the intervention was calculated per group, followed by the net therapeutic gain (REN minus placebo):
Acute medications intake
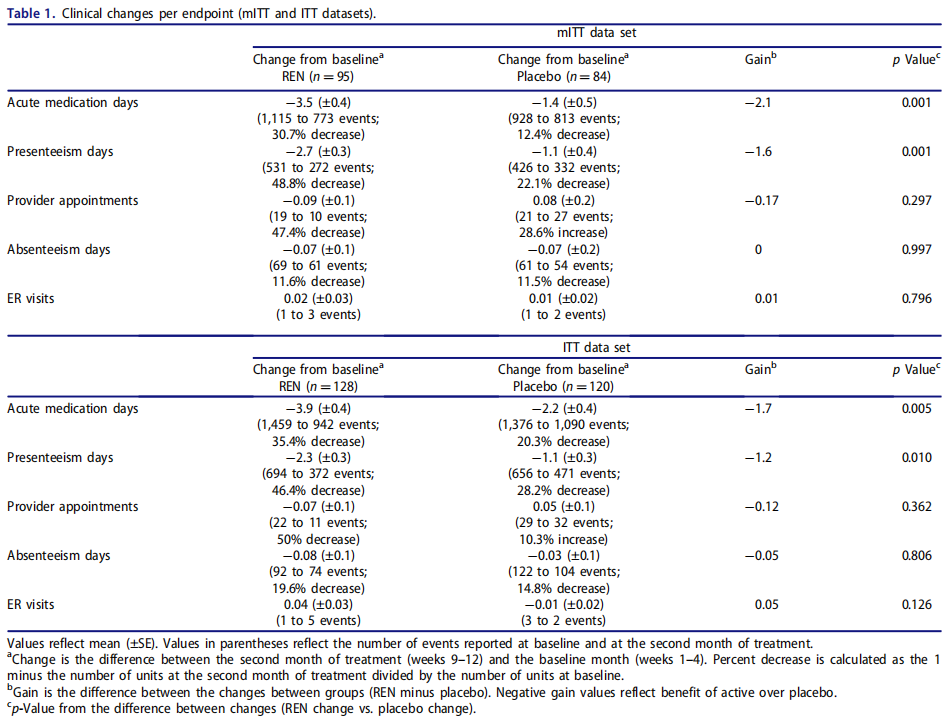
The groups significantly differed in the mean change in num- ber of days of acute medication treatments for headache/mi- graine from baseline to the last 4-weeks of treatment. Mean change in number of days of acute medication treatments was -3.4 (SE = 0.4) days in the REN group, vs. -1.2 (SE = 0.5) days in the placebo group. The net therapeutic gain was 2.2days; p = .001 (reduction in the active group: from 11.6 acute medication days at baseline to 8.2 at weeks 9–12; and from 11.0 to 9.8 in the placebo group); see Table 1.
Presenteeism
The groups significantly differed in the mean change in num- ber of presenteeism days, with a change of -2.7 (SE = 0.3) days in the REN group, vs. -1.1 (SE = 0.4) days in the pla- cebo group (net therapeutic gain of 1.6 days; active group: from 5.6 presenteeism days at baseline to 2.9 at weeks 9-12; placebo: from 5.1 to 4.0days; p= .001).
Provider appointments
There was no significant difference between groups in the change in number of healthcare provider appointments (p= .30). The mean change in number of healthcare provider appointments was -0.09 (SE = 0.1) in the REN group, and +0.08 (SE = 0.2) in the placebo group (active: from 0.20 mean appointments in baseline to 0.11 in weeks 9-12; pla- cebo: increase from 0.25 to 0.32). The number of HCP pro- vider visits was small (REN group: total of 19 visits reported by 15 participants at baseline, and 10 visits reported by 8 participants at weeks 9-12; placebo group: total of 21 visits reported by 17 participants at baseline, and 27 visits reported by 8 participants at weeks 9-12).
Absenteeism
There was no significant difference between groups in the change in absenteeism days (p= .997). The mean change in number of absenteeism days was -0.07 in both groups (p = .997; active: total of 69days reported by 32 participants at baseline, and 61days reported by 24 participants at weeks 9-12; placebo: total of 61days reported by 28 participants at baseline, and 54days reported by 26 participants at weeks 9-12).
ER visits, brain scans, inpatient admissions
There were no brain scans and no inpatient admissions dur- ing the study period, and the number of ER visits due to headache/migraine was very low (total of 7 events, ranging between 0 to 3 per group and phase). Therefore, data on these events were not included in the analyses. Summary of the clinical results is presented in Table 1, for both the mITT and ITT datasets.
Prophylaxis sub-analysis
Approximately 40% of the subjects used one preventive medication in addition to REN. The REN and placebo arms did not differ in the distribution of types of prophylactic medications (p= .41 in mITT, 0.24 in ITT).
The mean change in acute medication days in the no- prophylaxis sub-sample was -3.9 (SE = 0.4) in REN arm, vs. -1.4 (SE = 0.3) in the placebo arm; a net therapeutic gain of 2.5days; p = .0001. The mean change in presenteeism days in the no-prophylaxis sub-sample was -3.3 (SE = 0.2) in REN arm, vs. -1.3 (SE = 0.3) in the placebo arm; a net thera- peutic gain of 2.0days; p = .0001. All other endpoints did not significantly differ between the groups in the no-prophylaxis sub-sample ( Supplementary Appendix 2A).
In the prophylaxis sub-sample, the mean change in acute medication days was -2.7 (SE = 0.5), vs. -0.98 (SE = 0.3) in the placebo arm; a net gain of 1.7days; p = .002. The mean change in presenteeism days was -1.8 (SE = 0.3) in the REN arm, vs. -0.9 (SE = 0.3) in the placebo arm; net therapeutic gain of 0.9days; p = .0001. The mean change in provider appointments was -0.3 (SE = 0.1), vs. -0.03 (SE = 0.1) in the placebo arm; a net gain of 0.3 appointments; p = .005. All other endpoints were similar between the groups in the prophylaxis sub-sample ( Supplementary Appendix 2B).
Financial impact
Mean cost-savings from the adoption of REN for migraine prevention was calculated by comparing the change from baseline (i.e. without using REN) to the second month of REN treatment per endpoint and multiplying the change by the average unit cost. Table 2 presents cost-savings per end- point and total sum. The substantial uncertainty associated with each endpoint was reflected by the standard error of the mean (SE), accounting for variability around treatment effect estimates. Note that while there was no significant dif- ference between the active and placebo groups in the change in provider appointments and in absenteeism, there appeared to be a reduction within the REN group relative to baseline.
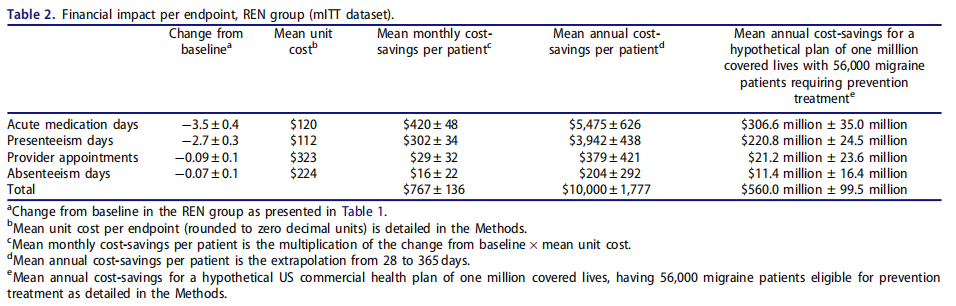
The aggregated annual cost savings for a plan covering a migraine patient treating with REN prevention is $10,000±1,777. This consists of $5,854±1,047 cost-savings from direct healthcare costs related to reduced consumption of acute medications and reduced provider appointments, and $4,146±730 cost-savings from indirect costs of lost pro- ductive time due to presenteeism. The annual cost savings for a hypothetical US commercial health plan of one million covered lives, with 56,000 members with migraine who should receive migraine prevention treatment (see Methods) is $560.0 million ± 99.5 million.
Similar savings are derived from the ITT dataset (mean annual savings of $9,987±1,777 per patient, mean annual savings for a hypothetical US commercial health plan of one million covered lives is $559.3 million ± 99.5 million; see Supplementary Appendix 3).The annual cost savings for a patient using REN as a standalone prevention treatment is $10,957±1,631, and $613.6 million ±91.3 million for a hypothetical US commercial health plan of one million covered lives. The annual cost sav- ings for a plan covering a migraine patient treating with REN in the prophylaxis sub-sample is $9,000±2,225 and $504.0 million ± 124.6 million for such a healthcare plan ( Supplementary Appendix 2).
For a plan that covers 56,000 migraine patients needing preventive treatment, the annual cost-savings is five hundred and sixty million dollars ($560.0 million ±99.5 million) from direct and indirect costs. The largest direct cost-savings con- stitutes a reduction of 2.5 million ± 292,000days of acute medications intake, translating to an average annual cost- savings of $306.6 million ± 35.0 million. An additional, yet smaller, source of reduced direct costs comes from a reduc- tion of 65,700±73,000 provider appointments following REN vs. Baseline, translating to an average cost-savings of $21.2 million ± 23.6 million. The occurrence of ER visits and brain- scans was too low to support a meaningful statistical ana- lysis. Thus, the total annual direct cost-saving for a hypothet- ical US commercial health plan of one million covered lives and 56,000 migraine patients needing migraine prevention treatment resulting from reduced acute migraine medica- tions and provider appointments is $327.8 million ±58.6 million.
The largest indirect cost-saving emerged from reduction in presenteeism, which is especially important for employers. Using REN prevention leads to a reduction of 35.2days of presenteeism per patient per year (equivalent to about 1.5 working months per year), and 0.91days of absenteeism per patient per year. Extrapolated over 56,000 employees per year, this constitutes a reduction of 1.97 million days of pres- enteeism in patients who treat with REN prevention relative to their baseline, translating to an average cost-savings of almost quarter billion dollars ($220.8 million ± 24.5 million). An additional, yet smaller, component of reduced indirect costs which are meaningful for employers comes from a reduction in absenteeism days following active treatment vs. baseline, which contributes to additional indirect cost-savings of more than 10 million dollars ($11.4 million ± 16.4 million) per year. The total annual indirect cost-saving derived from this study is 232 million dollars ($232.2 million ± 40.9 million).
Accounting only for the reduction in acute medications and presenteeism days, cost-savings would be $9,417±1,064 annually per patient, and more than half a billion dollars ($526.8 million ± 59.5 million) annual savings for a hypothet- ical US commercial health plan of one million covered lives.
Additional sub-analyses were conducted to assess the effects of gender and retirement age on presenteeism. The majority of the participants (86%) were within working-age, below the US retirement age of 62 years for males and females alike. Reduction in presentism after 2 months of intervention in subjects within working age was the same as for those of retirement age in each group (active group: working age presenteeism: -2.63±0.33, retirement age pres- enteeism: -3.07±1.04, p = .62; placebo group: working age presenteeism: -0.99±0.39,retirement age presenteeism:-1.74±0.64, p= .48). Regarding gender, in both groups the ratio of female:male was 86%:14%. Reduction in presentism after 2months of intervention was the same for females and males in each group (active group: female presenteeism:-2.51±0.34, male presenteeism: -3.85±1.02; p = .07; pla- cebo group: female presenteeism: -1.20±0.38, male present- eeism: -0.31±0.92; p= .18). Taken together, the economic benefit related to presenteeism is applicable for any age and for any gender group.
Discussion
Migraine imposes a considerable economic burden on patients, healthcare systems, and employers in the US. The results reported in this paper indicate a substantial reduction in both the clinical and the financial burden brought about by effective migraine preventive treatment using the REN (Nerivio) device, substantially mitigating losses both to health and economics. The results of eight weeks of REN pre- ventive treatment led to an average annual cost-savings of ten thousand dollars per patient ($10,000±$1,777) from both direct and indirect sources. Extrapolated to a hypothet- ical US commercial health plan of one million covered lives as often done in health economics evaluations, with 14.0% people with migraine, out of which 40% could bene- fit from prevention treatment, 56,000 plan members should receive migraine prevention treatment. For such a plan, the current analysis suggests clinical benefits that translate to cost-savings of more than half a billion dollars $560 million ± $99.5 million per year when using REN as preventive treat- ment, relative to costs when not using REN for preventive treatment. These savings are composed of $327.8 million- ±$58.6 million direct costs and $232.2 million±$40.9 million indirect costs.
These results are in line with population-based studies in North America demonstrating the main contribution of pres- enteeism to the loss of productivity. Patients and employ- ers alike would thus stand to benefit from preventive migraine treatments that significantly improve productivity such as REN.
While this is the first study to assess and demonstrate cost-saving from REN treatment, a number of study limita- tions should be acknowledged. First, several of the endpoints had only scarce occurrences (absenteeism days, provider appointment, and ER visits) or were not at all reported (brain scans and inpatient admissions), limiting the chances of iden- tifying between-groups differences. Not surprisingly, provider visits are more common than ER visits and brain scans in people with migraine5. A longer study is expected to have higher occurrences of such events, allowing better assess- ment of the clinical and financial impact of these parameters.
Second, the number of provider appointments and absen- teeism days following two months of intervention did not significantly differ between REN and placebo. Yet the lack of between-groups significance does not negate the contribu- tion and importance of cost-savings from changes in these endpoints in the REN group. In real-world, there is no “placebo” treatment, and cost-savings results from covering a specific treatment relative to not covering that treatment. Thus, even though the difference between the groups in these two metrics (which had only scarce occurrences during the study) is not statistically significant, they provide eco- nomically meaningful cost-savings from utilizing REN for migraine prevention.
Third, while only a handful of US employers employ more than a million people, there are many commercial health plans that provide health insurance to multiple employers and thus overall cover millions of employees, making the extrapolation presented here relevant for them. Specific employers can assess the number of their employees that live with migraine and easily scale the cost-savings to their individual plan.
Forth, the cost-savings presented here might be conserva- tive, underestimating the full cost-savings from REN prevent- ive treatment. The current study only assessed cost-savings from endpoints measured during the clinical trial itself and did not include direct cost-savings from the different prices of REN vs. other non-generic preventive treatments available in the US which are more expensive. The study also did not evaluate the indirect costs from the psychological burden of migraine (including anxiety, depression, stress, catastrophiz- ing). Further research may provide the full cost-effective- ness/cost-utilization analysis aspects associated with using REN to prevent migraine, including acquisition-costs and other burdens.
Conclusions
This study indicates that use of the REN (Nerivio) device as a preventive treatment for migraine reduces disease burden and lowers the associated financial costs, both direct and indirect, across multiple domains. These findings amplify the clinical benefits from REN preventive treatment beyond those previously reported elsewhere. These findings further demonstrate the cost-saving value of REN preventive treat- ment, providing an incentive for patients,health insurance plans, and employers to closely assess the merit of using REN for migraine prevention. The significant presenteeism cost savings may be especially invaluable to large employers.
